Summary
- Overview
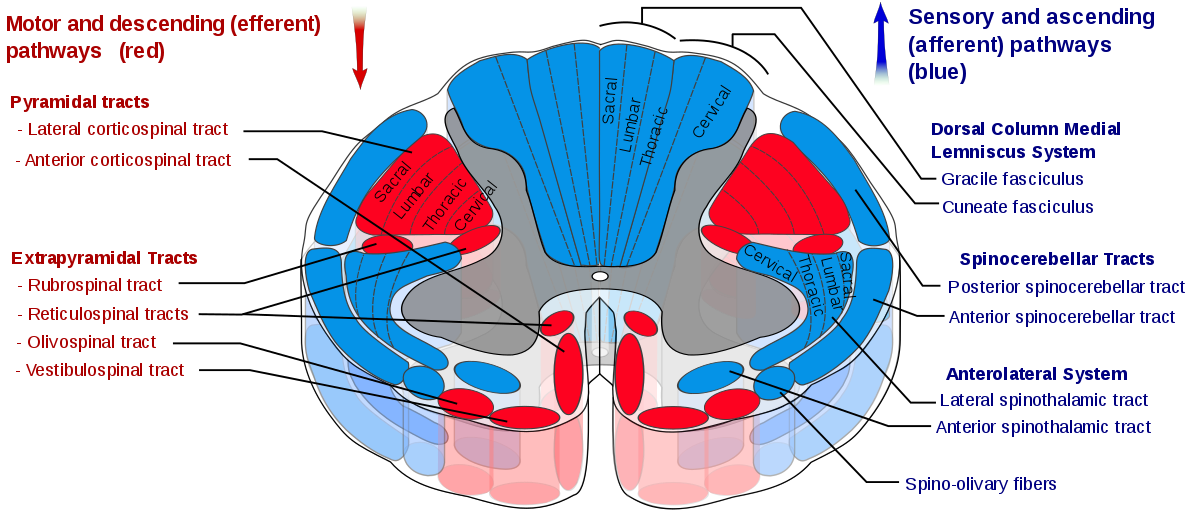
- The descending (motor) tracts:
- Pyramidal:
- Corticospinal
- Lateral corticospinal tract
- Anterior corticospinal tract
- Corticobulbar
- Corticospinal
- Extra-pyramidal:
- Tectospinal
- Vestibulospinal
- Rubrospinal
- Reticulospinal
- Olivospinal
- Pyramidal:
Summary Table

Overview of the Descending Tracts
- Required for control of:
- Skeletal muscle movement
- Muscle tone
- Spinal reflexes
- Modulation of sensory transmission
- Motor autonomic functions
- There are two types of tracts:
- Pyramidal – these are associated with voluntary movement
- Corticospinal – discrete voluntary movement of body
- Lateral corticospinal tract – limb muscles
- Anterior corticospinal tract – axial muscles
- Corticobulbar – voluntary movement of muscles of the face and neck (via cranial nerves)
- Corticospinal – discrete voluntary movement of body
- Extra-pyramidal – generally associated with postural tone
- Tectospinal – reflexes in response to visual stimuli
- Vestibulospinal – promotes antigravity action (stimulates extensors/inhibits flexors)
- Rubrospinal – promotes flexor activity of the upper limb
- Reticulospinal – modulates reflex activity
- Olivospinal
- Pyramidal – these are associated with voluntary movement
Corticospinal Tract
Structure
- Made up of 2 parts
- Lateral CT
- Ventral/Anterior CT
- Functions
- Control of discrete voluntary movements:
- Lateral CT – distal limb (especially flexors)
- Ventral/Anterior CT – Proximal/axial muscles
Innervates a-motor neurones only (unlike other tracts)\
- Some role in modulation of local reflexes
- Dampens down local reflexes
- Control of discrete voluntary movements:
- Pathway:
- UMN originates in 1o motor cortex
- Some fibres from 2o sensory cortex
- Fibres pass through the internal capsule
- Decussation
- 85% of fibres decussate at medulla – These become the lateral corticospinal tract
- Remaining 15% continue ipsilaterally as the medial/ventral corticospinal tract
- Medial tract decussates at level of synapse
- Both synapse with their LMN at the ventral horn of the spinal level where they exit
- 55% cervical
- 20% thoracic
- 25% lumbar
- (Most of the ventral corticospinal tract in particular terminates in thoracic spinal cord)
- UMN originates in 1o motor cortex

Corticobulbar tract
- Functions
- Controls muscles of face and neck
- Innervates bilaterally (except for lower facial nuclei)
- Directly controls CNV, CNVII, CNXII
- Indirectly controls CNIII, CNIV, CNVI (via interneurons)
- Controls muscles of face and neck
- Structure – see diagram
- Varies depending on each nerve

Tectospinal tract
- Functions:
- Contraction of neck muscles on contralateral side (toward stimulus)
- E.g. right TST contracts left neck muscles to turn head to the left
- Orientates head and neck to auditory/visual stimuli
- E.g. keeps head straight when bending over laterally
- Contraction of neck muscles on contralateral side (toward stimulus)
- Pathway:
- Originates from superior colliculus
- Rostral aspect of midbrain
- Receives visual and auditory afferents
- Decussates in dorsal tegmentum (also in midbrain)
- Descends ventromedially alongside medial vestibulospinal tract
- Predominantly terminates in cervical spinal cord
- Control muscles of head/neck
- Originates from superior colliculus

Vestibulospinal tracts
- 2 tracts:
- Lateral vestibulospinal tract (supplies lower limb)
- Medial vestibulospinal tract (supplies head and neck)
- Functions
- Antigravity action: stimulate extensors and inhibit flexors (of the legs/neck in particular) – remember as vestibular system being responsible for balance
- Lateral – Lower limb extension
- Medial – Neck extension
- Antigravity action: stimulate extensors and inhibit flexors (of the legs/neck in particular) – remember as vestibular system being responsible for balance
- Pathway
- Originate in vestibular nuclei in pons/medulla
- Lateral – Deiter’s nucleus (lateral vestibular nucleus)
- Medial – medial vestibular nucleus
- Receive afferent input from labrynthine system via CNVIII/cerebellum
- Do not decussate:
- Therefore remain ipsilateral
- Terminate in:
- Lumbar spine (lateral tract) => leg extensors
- Cervical spine (medial tract) => neck extensors
- Originate in vestibular nuclei in pons/medulla

Rubrospinal tract
- Functions:
- Maintains tone of limb flexors – inhibits anti-gravity extensors
- Particularly arm
- Essentially opposite in function to the vestibulospinal tracts
- Maintains tone of limb flexors – inhibits anti-gravity extensors
- Pathway
- Originates in red nucleus (in midbrain tegmentum)
- Descends ventromedially
- Decussates in ventral tegmentum
- Becomes ventrolateral after decussation
- Terminates in cervical and lumbar spine
- Only innervates limb LMNs

Reticulospinal
- 2 parts:
- Medullary RST => excites antigravity extensors (like vestibulospinal)
- Pontine RST => inhibits antigravity extensors (like rubrospinal)
- Other functions
- Modulates voluntary movement and muscle tone
- Modulates CVS
- Modulates pain impulses
- Mediates autonomic functions
Decorticate + Decerebrate lesions
- A key phenomenon is decortication
- This is where the upper limbs become flexed, and lower limbs extended
- Normally, arm extension is facilitated by:
- The vestibulospinal tracts
- The medullary reticulospinal tract
- Arm flexion is facilitated by
- The rubrospinal tract
- The pontine reticulospinal tract
- Normally suppressed by the corticospinal tract
- With an injury above the brainstem, the the tracts responsible for arm flexion are disinhibited (due to loss of the corticospinal tract) and overcome those causing arm extension
- With decerebrate lesions (i.e. the brainstem is also involved), the rubrospinal tract is also lost. Therefore, an extension posture can develop